Screening Emergency Department Patients with Chest Pain Symptoms Using Coronary CT Angiography
In This Article
- Magnetoencephalography can detect neuronal activity noninvasively by measuring the magnetic fields surrounding the human head
- Every year in the U.S., as many as eight million patients present to emergency departments with chest pain symptoms
- Current approaches to triaging these patients often include admitting them to the hospital for observation and testing at considerable time and expense
- Research has established coronary computed tomography angiography as a safe and effective alternative to the current strategy of admission for observation, stress tests and/or myocardial perfusion imaging stress tests
Chest pain is one of the most common reasons for emergency department (ED) visits among adults in the U.S., with upwards of eight million patients presenting every year with chest pain symptoms. EDs devote considerable resources to screening these patients for acute coronary syndromes (ACS). However, only 10 to 15% of low-risk patients who present with chest pain are ultimately diagnosed with ACS. The noninvasive imaging modality coronary computed tomography angiography (CCTA) offers a means to evaluate these patients both safely and efficiently, with shorter discharge times and similar or reduced costs.
Subscribe to the latest updates from Radiology Advances in Motion
CCTA Offers Advantages Over Standard Evaluation for Triage of Emergency Department Patients Suspicious for Acute Coronary Syndrome
For many years, providers triaged ED patients presenting with chest pain based on medical history, serial electrocardiogram (ECG) recordings and measurement of biomarkers. While this approach proved acceptable, the risks of undetected ACS were ultimately too great. Two percent or more of the patients discharged after triage without further tests or treatment were later diagnosed with ACS. This delay in diagnosis resulted in higher mortality rates for these patients.
To limit the number of ACS cases missed in the ED, many institutions adopted a “rule-out myocardial infarction” strategy using admission for observation stress tests and/or myocardial perfusion imaging (MPI) stress tests to determine narrowing or blockage of the arteries. While this approach led to a reduction in errors in the diagnosis of ACS, it also brought about a dramatic increase in time and resources to triage patients presenting with chest pain, especially since most providers admit these patients to the hospital for testing. Research suggests diagnosis of chest pain in the ED now costs an estimated $10 to $12 billion per year in the U.S., partly due to implementation of this strategy. Much of this financial burden reflects societal costs beyond direct health expenditures, such as missed days of work for patients admitted to hospitals.
CCTA, which produces three-dimensional images of the arteries delivering blood to the heart by scanning a patient during injection of a contrast agent, can help to more efficiently triage patients with suspicion for ACS. In a series of randomized trials over the past decade, researchers explored the potential of CCTA in the ED. In a 2012 study reported in the New England Journal of Medicine, a team of investigators led by Massachusetts General Hospital radiologists compared a CCTA-based strategy to standard evaluation and showed it had a significantly shorter average hospital stay and time to diagnosis, as well as higher rates of direct discharge from the ED. The new strategy was associated with more diagnostic testing and radiation exposure, but the researchers found no greater risk of undetected ACS and no increases in the overall cost of care. A 2011 study in the Journal of the American College of Radiology compared CCTA to a strategy including myocardial perfusion imaging, and CCTA was associated with lower costs and radiation exposure as well as greater safety and efficiency benefits.

Figure 1
Mass General radiologist Brian B. Ghoshhajra, MD, and colleagues have described the benefits of implementing CCTA in the ED to evaluate patients presenting with chest pain symptoms.
Implementation of CCTA in Clinical Practice Suggests Additional Benefits, Including Reduced Radiation Exposure
Many randomized trials over the past decade have shown CCTA to be a safe and efficient means of triaging patients presenting to the ED with suspicion for ACS, with shorter disposition times and similar or reduced costs compared to standard of care. Researchers at Mass General recently demonstrated the safety and efficiency of its clinical application in a 2017 issue of European Radiology. The study reported the clinical implementation of a CCTA protocol for triage of ED patients with suspicion for ACS and included an analysis of a three-year registry that tracked 1,022 consecutive patients. The analysis showed that the protocol not only agreed with but in some cases also improved upon the results of previously reported randomized trials. For example, using the newest, most advanced CT systems and the latest software, the researchers showed they could reduce radiation dose by more than 50% compared to earlier trials. The authors suggested that the safety and efficiency of the protocol will further increase as clinical teams in the ED and hospital grow more familiar with CCTA technology.
More recently, members of the Mass General team have shown that CCTA can also play a role in diagnosing intermediate-to-high-risk ED patients with suspicion for ACS. The number of these patients is expected to increase as the U.S. population ages. In a letter published last year in JACC: Cardiovascular Imaging, the researchers reported that CCTA could provide a safe and effective means of detecting or excluding coronary artery disease (CAD) in patients with elevated risk of ACS. An analysis of the previously established CCTA registry, which grew to include 2,290 ED patients who had undergone CCTA between October 2012 and March 2017, showed that the technique ruled out significant CAD in roughly two-thirds of the patients and demonstrated a negative predictive value of 97% for ACS. The researchers suggest that the noninvasive CCTA could serve as a “gate-keeper” for invasive coronary angiography (ICA) even in these higher risk patients, helping to reduce the number of unnecessary cardiac tests for the patients.
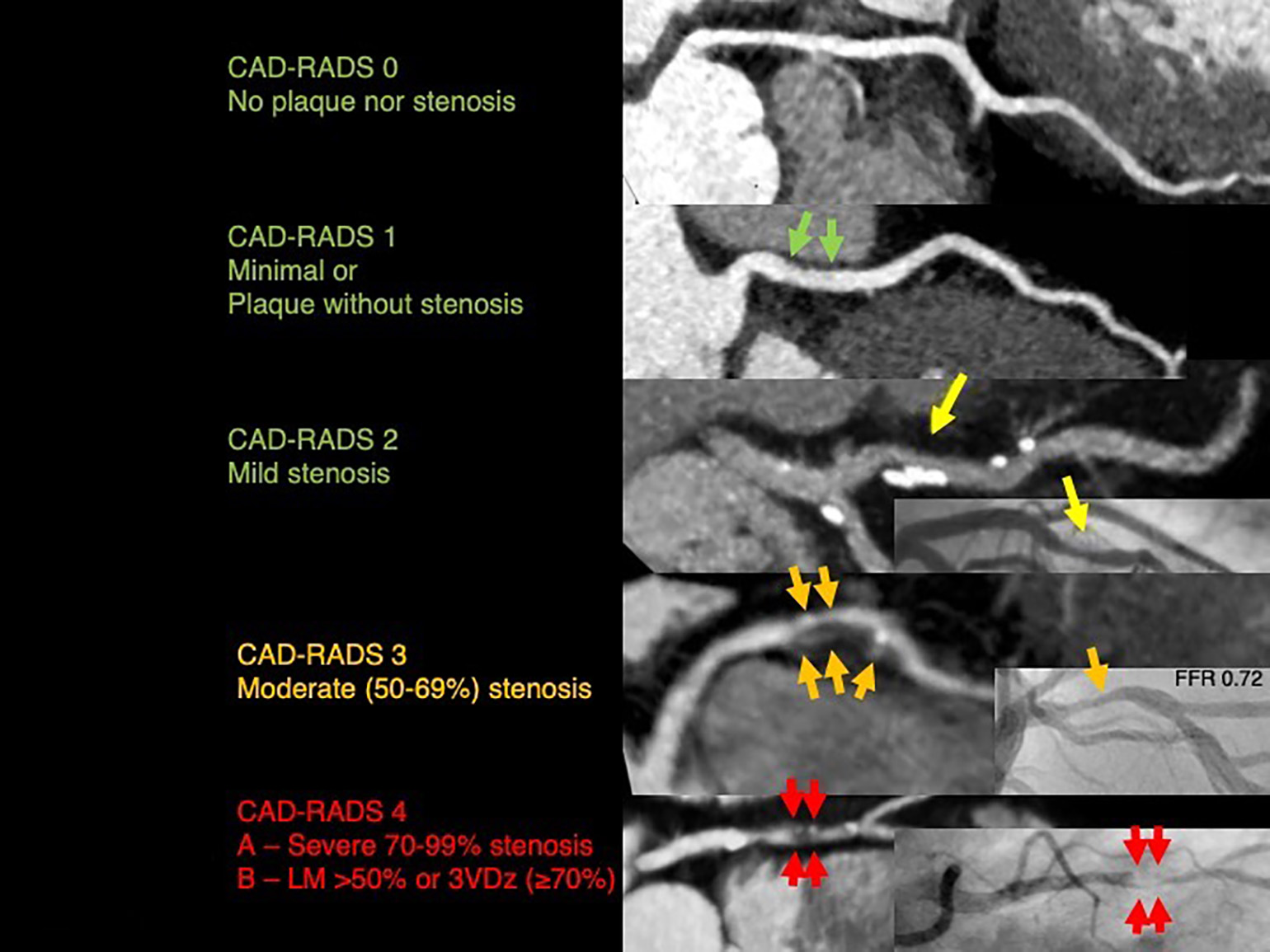
Figure 2
Shown here are scans of patients presenting with acute chest pain, negative first troponin, negative or nondiagnostic electrocardiogram and low to intermediate risk (TIMI risk score <4) (emergency department or hospital setting).
- CAD-RADS 0: ACS highly unlikely. No further evaluation of ACS is required. Consider other etiologies.
- CAD-RADS 1: ACS highly unlikely. Consider evaluation of non-ACS etiology, if normal troponin and no ECG changes. Consider referral for outpatient follow-up for preventive therapy and risk factor modification
- CAD-RADS 2: ACS unlikely. Consider evaluation of non-ACS etiology, if normal troponin and no ECG changes. Consider referral for outpatient follow-up for preventive therapy and risk factor modification
- CAD-RADS 2: ACS unlikely. Consider evaluation of non-ACS etiology, if normal troponin and no ECG changes. Consider referral for outpatient follow-up for preventive therapy and risk factor modification
- CAD-RADS 3: ACS possible. Consider hospital admission with cardiology consultation, functional testing and/or ICA for evaluation and management. Anti-ischemic and preventive management should be considered as well as risk factor modification. Other treatments should be considered if presence of hemodynamically significant lesion.
- CAD-RADS 4A or 4B: ACS likely. Consider hospital admission with cardiology consultation. Further evaluation with ICA and revascularization as appropriate. Anti-ischemic and preventive management should be considered as well as risk factor modification.
- CAD-RADS 5: ACS very likely. Consider expedited ICA on a timely basis and revascularization if appropriate if acute occlusion. Anti-ischemic and preventive management should be considered as well as risk factor modifications. Scheduling Non-ED CCTA is offered on the main campus of Massachusetts General Hospital in Boston. Orders can be placed in Epic (inside the Partners network) or Physician Gateway (outside the Partners network) or by calling 617-726-8396
References
- Goldstein JA, Chinnaiyan KM, Abidov A., et al. (2011). The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J Am Coll Cardiol 58(14): 1414-22.
- Litt HI, Gatsonis C, Snyder B, et al. (2012). CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med 2012 366: 1393-1403.
Learn more about the Division of Cardiovascular Imaging
Visit Mass General Imaging