Cardiac CT for the Characterization of an Intra-atrial Lesion
In This Case Study
- A 47-year-old with a history of a childhood posterior fossa cyst complicated by hydrocephalus requiring a ventriculo-peritoneal shunt and five subsequent revisions was transferred to MGH for the evaluation of one month of left sided hemianopsia and one week of headache and fevers
- Further evaluation included non-contrast head computed tomography (CT), which demonstrated a remote cerebrovascular accident (CVA) in the distribution of the right posterior communication artery and possible hydrocephalus and a chest radiograph, which revealed a right hilar mass
- CT of the chest, abdomen and pelvis demonstrated extensive and diffuse thoracic and abdominopelvic lymphadenopathy
- To better characterize the findings of the atrial mass on TTE, an ECG-gated contrast-enhanced cardiothoracic CT was requested
Subscribe to the latest updates from Cardiovascular Advances in Motion
Clinical History
A 47-year-old with a history of a childhood posterior fossa cyst complicated by hydrocephalus requiring a ventriculo-peritoneal shunt and five subsequent revisions (most recently in 1990) was transferred to MGH for the evaluation of one month of left sided hemianopsia and one week of headache and fevers.
Initial laboratory values demonstrated acute kidney injury, transaminitis and elevated lactate dehydrogenase. Further evaluation included non-contrast head computed tomography (CT), which demonstrated a remote cerebrovascular accident (CVA) in the distribution of the right posterior communication artery and possible hydrocephalus, and a chest radiograph, which revealed a right hilar mass.
Lumbar puncture demonstrated no evidence of increased opening pressure or meningitis.
CT of the chest, abdomen and pelvis demonstrated extensive and diffuse thoracic and abdominopelvic lymphadenopathy.
Oncology was consulted for guidance given the suspicion of malignancy; in anticipation of expediting treatment with chemotherapy, a transthoracic echocardiogram (TTE) was simultaneously requested to assess left ventricular function.
Flow cytometry of the blood was unrevealing and viral studies demonstrated positive heterophile antibody and Epstein-Barr virus (EBV) polymerase chain reaction. Cardiac ultrasound demonstrated preserved left and right ventricular function, but a 1.3 x 0.8 cm mass of echoes was identified in the right atrium on the lateral tricuspid annulus.
There was mild resultant obstruction to flow across the tricuspid valve (Figure A).
Given the suspicion for malignancy, concern for an unknown primary malignancy with cardiac invasion was raised. In order to further evaluate this concern for malignancy, a left inguinal excisional lymph node biopsy was pursued. To better characterize the findings of the atrial mass on TTE, an ECG-gated contrast-enhanced cardiothoracic CT was requested.
Findings
A previously undocumented abandoned ventriculoatrial shunt that terminated in the right atrium was discovered (the proximal shunt was discontinuous in the upper chest wall, and a contralateral intact ventriculoperitoneal shunt was also identified). The aforementioned mass was depicted as partially calcified and distinct from but adjacent to the shunt, located along the posterior aspect of the right atrial wall and tricuspid valve (Figures B, D). There was evidence of retraction of the atrial wall with minimal adjacent pericardial fluid; no evidence for endocarditis was identified. A patent foramen ovale was demonstrated, with left-to-right shunting.
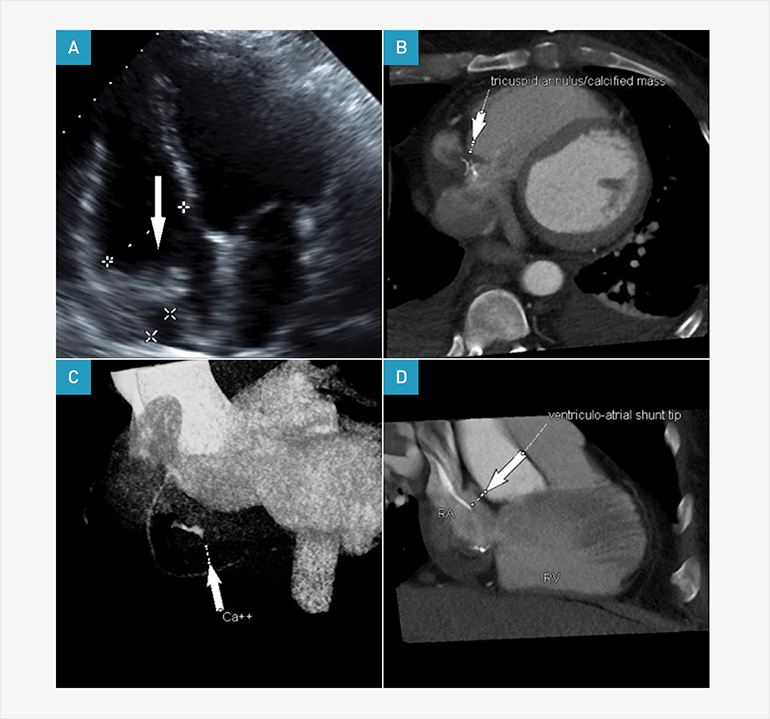
ECG-gated computed tomography (top left and right, bottom left) and transthoracic echocardiography (bottom right) images of a right atrial thrombus. (A) Cardiac ultrasound demonstrates a right atrial mass of echoes at the right atrioventricular groove (arrow) causing moderate obstruction of flow to the right ventricle with focal echobright areas with associated acoustic shadowing consistent with focal calcification. (B,C) Axial and 3D volume-rendered CT images demonstrate a partially calcified mass with low attenuation components (arrows) adjacent to the right atrial wall and (D) tricuspid valve that was distinct from but adjacent to the ventriculoatrial shunt (arrow).
Discussion
Although cardiac magnetic resonance imaging is often preferred for cardiac mass evaluation, cardiac CT also provides high-resolution morphological characterization of intracardiac masses in patients for whom echocardiography was not diagnostic. ECG-gated cardiac CT rapidly demonstrates anatomic relationships, assesses for the presence of calcium and evaluates soft tissue characteristics with the addition of intravenous contrast. Multiphase cardiac CT provides cine images that can be used to determine mass mobility and clarify dynamic anatomic relationships. Characteristic CT appearances of both benign and malignant intracardiac masses have been well described by location, structure and enhancement. Given the findings of a mass with low attenuation that respects anatomic boundaries and contains foci of calcification and proximity to a chronic indwelling intravascular catheter, this patient’s mass was diagnosed as a chronic catheter-associated thrombus via the CT findings.
Prior to discharge, the patient underwent a follow up TTE with agitated saline, confirming the patent foramen ovale. Pathology from the lymph node biopsy returned with immature and mature B cells that stained positively for EBV. Ultimately, it was felt that his fever and lymphadenopathy were consistent with acute EBV infection and that he would continue to recover with supportive therapy. Given evidence of a prior CVA, medical therapy was instituted with consideration for anticoagulation, given the possibility of paradoxical embolism from the tricuspid valve thrombus.
References
- Wintersperger BJ, Becker CR, Gulbins H, Knez A, Bruening R, Heuck A, Reiser MF. Tumors of the cardiac valves: imaging findings in magnetic resonance imaging, electron beam computed tomography, and echocardiography. Eur Radiol. 2000;10(3):443-9.
- Hoey ET, Mankad K, Puppala S, Gopalan D, Sivananthan MU. MRI and CT appearances of cardiac tumours in adults. Clin Radiol, 2009;64(12):1214-30.
- Bolster F, Fardanesh R, Morgan T, Katz DS, Daly B. Cross-sectional imaging of thoracic and abdominal complications of cerebrospinal fluid shunt catheters. Emerg Radiol. 2016;23(2): 117-25.