Cardiac CT Mechanical Valve Prosthesis Dysfunction Diagnosis
In This Case Study
- A 27-year-old woman with history of type 1 truncus arteriosus presented with several months of progressive dyspnea for subspecialty ACHD care
- Cardiac MR confirmed a dilated right ventricle with moderately depressed ejection fraction (RVEF 35%) and identified pulmonary artery stenosis
- Cardiac CT confirmed a stenosis of the left and right pulmonary arteries and cine images depicted a mechanical failure of the artificial pulmonic valve
- Surgical replacement of the mechanical pulmonic valve as well as reconstruction of the main pulmonary arteries resulted in the resolution of symptoms
- Cardiac CT is the test of choice for detecting thrombus formation and evaluating mechanical valve dysfunction
Clinical History
A 27-year-old woman with history of type 1 truncus arteriosus presented with several months of progressive dyspnea for subspecialty adult congenital heart disease care. Prior correctional procedures included:
Subscribe to the latest updates from Cardiovascular Advances in Motion
- Placement of a right ventricle to pulmonary artery conduit at age 2 months
- Homograft conduit replacement at ages 6 and 14
- Pulmonary artery bifurcation stenting at age 7
- Placement of St. Jude aortic and pulmonic valves at age 14
Physical examination was notable for a harsh right ventricular outflow tract conduit murmur and a short diastolic murmur consistent with pulmonic regurgitation. Outside cardiac ultrasound was interpreted to show right ventricular dilatation and dysfunction, and suggested a paravalvular pulmonic leak. Cardiac magnetic resonance (MR) at Massachusetts General Hospital confirmed a dilated right ventricle with moderately depressed ejection fraction (RVEF 35%) and identified pulmonary artery stenosis. In consideration for possible percutaneous pulmonary artery intervention, ECG-gated cardiac CTA was requested.
Findings
Cardiac CT confirmed a stenosis of the left and right pulmonary arteries; no evidence of paravalvular leak was identified. Additionally, cine images depicted a mechanical failure of the artificial pulmonic valve, with the two flaps fixed in the open position throughout the cardiac cycle, caused by thrombus adherent to the left prosthetic valve leaflet. Total exam dose (including whole-chest non-contrast and cine contrast-enhanced imaging) was 6.5 mSv. Because this was an unsuspected finding, and cardiac ultrasound was non-diagnostic (acoustic windows were limited), cine fluoroscopy was performed, confirming that the prosthetic pulmonic valve was fixed in the open position. Surgical replacement of the mechanical pulmonic valve as well as reconstruction of the main pulmonary arteries was performed, with resolution of symptoms.
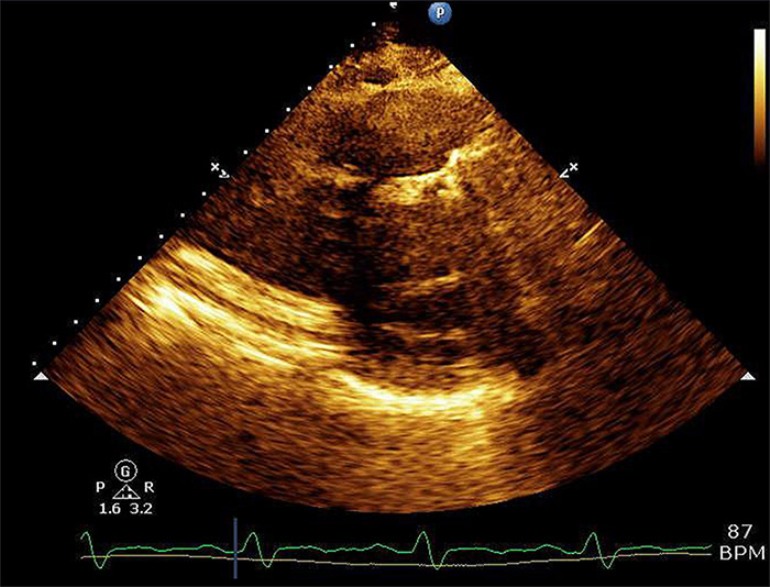
Figure A.
Outside echocardiography (oblique parasternal view) of the pulmonic valve prosthesis was limited by significant shadowing artifact from the prosthetic valve leaflets.
Figure B.
ECG-gated CTA multiphase thick MPR and volume rendered (upper right) reformats illustrates normal opening of the leaflets of a well-seated mechanical aortic valve.
Figure C.
ECG-gated CTA multiphase thick MPR and volume rendered (upper right) reformats illustrates fixed position of the leaflets of the artificial pulmonic valve leaflets, with no significant motion throughout the cardiac cycle. Additionally, there is a low density thrombus adherent to and obstructing the base of the left pulmonic valve leaflet (lower left).
Figure D.
Fluoroscopic cine imaging of the artificial aortic and pulmonic valves confirms normal motion of the aortic valve leaflets, and fixed position of the pulmonic valve leaflets.
Discussion
While most patients undergo pulmonary valve replacement with a tissue valve, the more durable mechanical valve can also be used, which necessitates permanent systemic anticoagulation. The incidence of mechanical valve failure has ranged from 8% - 18% in multiple studies, with most failures secondary to thrombosis formation. The excellent spatial resolution of CT coupled with the ability to acquire dynamic images with ECG gating, and ability to reconstruct images in any plane, makes cardiac CT the test of choice for detecting thrombus formation and evaluating mechanical valve dysfunction with the lowest radiation dose possible. Although ultrasound is the primary test of choice for valvular function, in this case the evaluation was limited by difficult acoustic windows and prior surgical material. MRI, while offering additional information via phase-contrast imaging, MRA, and unrestricted imaging planes, can be limited at the site of the valve itself, as in this case, by local distortion of the magnetic field, particularly in metallic valves.
References
- Dehaki MG, Ghavidel AA, Omrani G (2015) Long – Term Outcome of Mechanical Pulmonary Valve Replacement in 121 Patients with Congenital Heart Disease. Thorac Cardiovasc Surg. 2015 Aug; 63 (5): 367-72 (PMID 25184609).
- Sadeghpour A, Kyavar M, Javani B, et al. (2014) Mid – Term Outcome of Mechanical Pulmonary Valve Prostheses: The Importance of Anticoagulation. J Cardiovasc Thorac Res. 2014; 6 (3): 163-8 (PMID 25320663).
- Saremi, F., Gera, A., Ho, S. Y., Hijazi, Z. M., & Sánchez-Quintana, D. (2014). CT and MR imaging of the pulmonary valve. Radiographics: a Review Publication of the Radiological Society of North America, Inc. 34(1), 51–71. http://doi.org/10.1148/rg.341135026.
- Ueda, T., Teshima, H., Fukunaga, S., Aoyagi, S., & Tanaka, H. (2013). Evaluation of prosthetic valve obstruction on electrocardiographically gated multidetector-row computed tomography--identification of subprosthetic pannus in the aortic position. Circulation Journal: Official Journal of the Japanese Circulation Society. 77(2), 418–423.
- Richau, J., Dieringer, M. A., Traber, J., Knobelsdorff-Brenkenhoff, von, F., Greiser, A., Schwenke, C., & Schulz-Menger, J. (2017). Effects of heart valve prostheses on phase contrast flow measurements in Cardiovascular Magnetic Resonance – a phantom study. J Cardiovasc Magn Reson. 19(1), 5. http://doi.org/10.1186/s12968-016-0319-1.
Visit Mass General Department of Radiology Imaging
Visit the Mass General Heart Valve Program