Mechanical Ventilation in the Era of COVID-19: An Ongoing Debate
The FLARE Four
- Current knowledge of COVID-19 is largely based on descriptive case series and anecdotal experience
- The description of purported “phenotypes” of COVID-19 patients has led to vigorous debate about mechanical ventilation strategies
- COVID-19 patients represent a spectrum of disease, just as other etiologies of ARDS, and resemble historic non-COVID cohorts in their respiratory mechanics
- Future directions examining long-term outcomes in patients with COVID-19 are necessary next steps
Many people are saying...we need more data before making practice-changing decisions in COVID-19 ARDS management.
Subscribe to the latest updates from FLARE Advances in Motion
Introduction
Coronavirus 2019 (COVID-19) has created much debate in the critical care world regarding a slew of management decisions, including sedation, proning, and mechanical ventilation strategies. To date, much of this debate has been limited to anecdotal experiences and case series.
A New Case Series Involving Mechanically Ventilated Patients with COVID-19
A recent study by a group from Massachusetts General Hospital and Beth Israel Deaconess Medical Center highlights outcomes in 66 mechanically ventilated patients with COVID-19 (Ziehr et al. 2020). All patients were mechanically ventilated with a median age of 58 years, nearly 7 out of 10 were male, one-third current or former smokers, roughly half had hypertension, and nearly one quarter had diabetes.
After intubation, modest positive end expiratory pressure (PEEP) was utilized (median 10 cm H2O; IQR 8-12), with goal plateau pressures (median 21; IQR 19-26), and lower dead space fractions (median 0.45; IQR 0.38-0.58). Roughly half underwent prone positioning with improvement in compliance and oxygenation. One-third were exposed to paralytic agents.
With a median follow-up of 34 days, roughly 6 out of 10 patients were liberated from mechanical ventilation, 3 out of 4 left the ICU, and 1 in 6 died.
How Does the Recent Case Series Compare to Prior Cohorts?
The recently published cohort by Ziehr et al. represents the largest, most systematic survey to date of respiratory mechanics in patients with COVID-19. Whereas early anecdotes prompted speculation that COVID-19 patients may have preserved respiratory mechanics relative to non-COVID ARDS patients, lung compliance was reduced in this cohort (35 mL/cm H2O), comparable to another recent COVID-19 cohort (Bhatraju et al. 2020). Patients underwent proning more frequently compared to those in the Italian cohort (Grasselli et al. 2020). In addition, mortality in this mechanically ventilated cohort was much lower (16.7%) than previously described, ranging from 25%-50% (Bhatraju et al. 2020, Grasselli et al. 2020). As heated high flow nasal cannula was not available, it is possible that patients were intubated with lower severity of illness and therefore more likely to survive compared to other cohorts.
Another strength of the manuscript by Ziehr et al. is the addition of complete information on mechanical ventilation. While multiple studies have been published capturing different centers’ experiences with COVID-19 patients, extrapolating and understanding the severity of ARDS and the outcomes of patients who were mechanically ventilated is less clear (Table 1). While some case-series clearly delineate the details of ICU admissions, others are less clear.
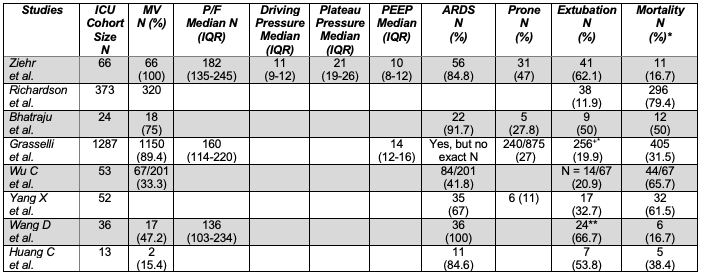
Table 1
Case-series manuscripts reviewed which encompassed ICU stays.
ICU: Intensive care unit; MV: Mechanical ventilation; P/F: PaO2/FiO2; PEEP: peak end-expiratory pressure; ARDS: acute respiratory distress syndrome
**This assumes patients are not mechanically ventilated on general medicine wards.
* Mortality ranges are a likely reflection of differences in disease severity, comorbidities, and censoring times (i.e. follow-up periods).
+ This assumes patients not in the ICU have been extubated.
How Does this Case Series Influence the Debate of COVID-19 Phenotypes and Mechanical Ventilation Strategy?
There has been much debate about the so-called L (low) and H (high) COVID-19 ARDS phenotypes (Gattinoni et al. 2020; Marini & Gattinoni 2020). Some have argued that the two suggested phenotypes require different treatment strategies, the L-type requiring typical low tidal volume ventilation settings, and the H-type requiring higher tidal volume and lower PEEP. To date, data supporting the existence of these phenotypes has been lacking, confined to a single case series of 16 patients, with a normally distributed range of lung compliance values (Gattinoni et al. 2020). Further, no randomized data support the claim that mechanical ventilation strategies should be altered based on features of these purported phenotypes.
One of the more interesting assets of the recent study by Ziehr et al. is Figure 1, which demonstrates the PaO2:FiO2 ratio, plateau pressure, PEEP, and static compliance over the first 5 days of mechanical ventilation (Ziehr et al. 2020). From this figure, it would be hard to define two different phenotypes by arbitrary single value cutoffs. The patients are representative of a wide array of compliance. We find it difficult to group patients into L and H phenotypes.
Importantly, the clinicians in the current study did not alter their mechanical ventilation strategies as compared to non-COVID ARDS patients, yet they attained favorable outcomes relative to prior reports. Based on this experience, there is no reason to suspect that conventional management strategies (including low tidal volume ventilation and traditional PEEP strategies) are harmful for COVID patients.
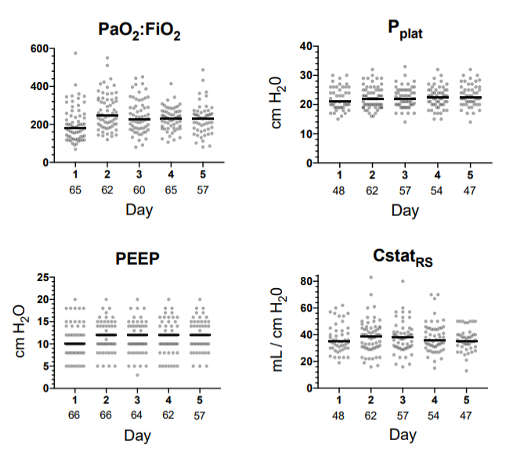
Figure 1
Respiratory Indices During the First Five Days of Mechanical Ventilation (Ziehr et al. 2020).
Limitations
The lack of heated high flow oxygen use in this cohort, lack of demographic information regarding race, and the lack of complete outcomes data due to the follow-up period are limiting factors in interpretation and generalization of this data to other populations.
Conclusions
Ziehr et al. have made a valuable contribution to the COVID-19 literature, sharing the most comprehensive report to date of respiratory mechanics in COVID patients. Their data do not support the existence of distinct phenotypes of COVID patients, suggesting instead that their lung compliance exists on a continuum comparable to non-COVID ARDS patients. Use of conventional mechanical ventilation strategies for ARDS are compatible with relatively favorable ICU outcomes in COVID patients. The focus of future efforts should systematically examine how centers are treating patients with COVID-19 and measuring long-term outcomes in these patients.
References:
- Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S, Chiumello D. Covid-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. Published online March 30, 2020. doi:10.1164/rccm.202003-0817LE
- Gattinoni L, Chiumello D, Caironi P, et al. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med. Published online April 14, 2020. doi:10.1007/s00134-020-06033-2
- Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in Critically Ill Patients in the Seattle Region - Case Series. N Engl J Med. Published online March 30, 2020. doi:10.1056/NEJMoa2004500
- Grasselli G, Zangrillo A, Zanella A, et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA. Published online 06 2020. doi:10.1001/jama.2020.5394
- Marini JJ, Gattinoni L. Management of COVID-19 Respiratory Distress. JAMA. Published online April 24, 2020. doi:10.1001/jama.2020.6825
- Richardson S, Hirsch JS, Narasimhan M, et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. Published online April 22, 2020. doi:10.1001/jama.2020.6775
- Ziehr DR, Alladina J, Petri CR, et al. Respiratory Pathophysiology of Mechanically Ventilated Patients with COVID-19: A Cohort Study. Am J Respir Crit Care Med. Published online April 29, 2020. doi:10.1164/rccm.202004-1163LE
- Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. Published online February 24, 2020. doi:10.1016/S2213-2600(20)30079-5
- Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. Published online February 7, 2020. doi:10.1001/jama.2020.1585
View all COVID-19 updates
Learn more about research in the Division of Pulmonary and Critical Care Medicine