Use of "Light Pipe" During Endoscopic Dacryocystorhinostomy No Substitute for Landmark-based Surgery
Key findings
- The maxillary line and axilla of the middle turbinate are reliable landmarks from which to identify the location of the lacrimal sac along the lateral nasal wall during endoscopic dacryocystorhinostomy (endo-DCR)
- Still, many surgeons transitioning from external DCR to endo-DCR use an endocanalicular "light pipe" to transilluminate the lacrimal sac endonasally and guide placement of the osteotomy
- In this chart review of 39 endo-DCR procedures that included lacrimal sac transillumination, the endoscopic point of transillumination was entirely posterior to the maxillary line in 82% of cases
- The light transilluminates through the thin posterior bone of the lacrimal sac fossa but not the thick anterior bone, which is the optimal location for osteotomy as it is away from adjacent structures and opens into a wider space within the nasal cavity
- This paper coaches oculoplastic surgeons about how to transition from external DCR to anatomic landmark–based endo-DCR and the benefits of collaborating with otolaryngologists
Advances in surgical instrumentation have prompted more oculoplastic surgeons to adopt an endoscopic approach to dacryocystorhinostomy (endo-DCR), a procedure that relieves nasolacrimal duct obstruction and tearing by creating a new pathway between the lacrimal sac and the nasal cavity.
Subscribe to the latest updates from Ophthalmology Advances in Motion
A critical step in successful endo-DCR is to locate the lacrimal sac correctly. Many surgeons transitioning from performing external DCR to endo-DCR use an endocanalicular "light pipe," such as a 23-gauge fiberoptic vitreoretinal endoilluminator, to transilluminate the lacrimal sac.
Daniel R. Lefebvre, MD, an oculoplastic surgeon in the Department of Ophthalmology at Mass Eye and Ear/Massachusetts General Hospital, initially used a light pipe as part of his standard endo-DCR protocol. However, he quickly realized relying on it could lead to inadequate osteotomy. In Orbit, he and colleagues describe the risks inherent in using a light pipe and outline precautions for surgeons learning endo-DCR.
Overview of a Troublesome Phenomenon
The maxillary line, an endonasal mucosal projection, is a reliable landmark from which to identify the location of the lacrimal sac. The line extends from the anterior middle turbinate attachment down along the lateral nasal wall to the dorsum of the inferior turbinate. It corresponds to the suture between the frontal process of the maxilla and lacrimal bone extranasally and the root of the uncinate process intranasally.
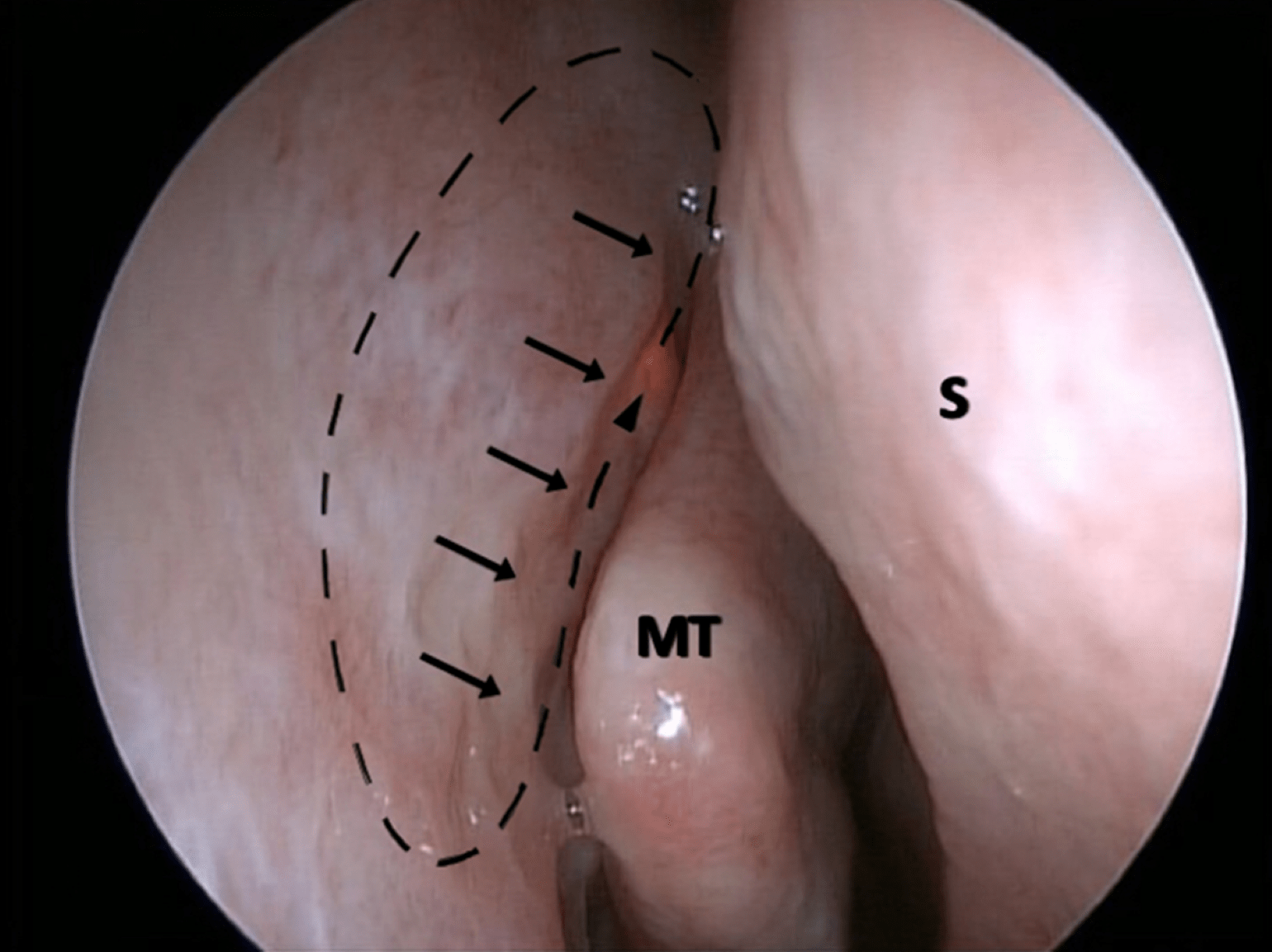
Figure 1
Intraoperative endoscopic view during endo-DCR surgery showing transillumination (arrowhead) completely posterior to the maxillary line (arrows). The planned DCR osteotomy is outlined by the dashed ovoid which overlies the anterior lacrimal sac fossa / frontal process of the maxilla. MT = middle turbinate; S = nasal septum.
However, during endo-DCR with a light pipe, the maxillary line and anterior are rarely transilluminated because the bone of the frontal process of the maxilla is substantially thicker than the lacrimal bone. Further, in some patients, the light signal is weakened because an agger nasi air cell is interposed over the upper part of the lacrimal sac.
If the maximum point of transillumination is posterior to the maxillary line, and only the illuminated area is targeted for bone removal, a novice surgeon would place the osteotomy in the incorrect position: under the middle turbinate within the middle meatus. Yet, removing the thicker bone present anteriorly and superiorly is critical to endo-DCR success. By biasing the DCR osteotomy anteriorly, the risk of DCR ostium to middle turbinate synechia formation is lessened; the potential need for middle turbinoplasty/turbinectomy is essentially obviated; and the risk of sinus outflow obstruction from scarring within the middle meatus is greatly lessened.
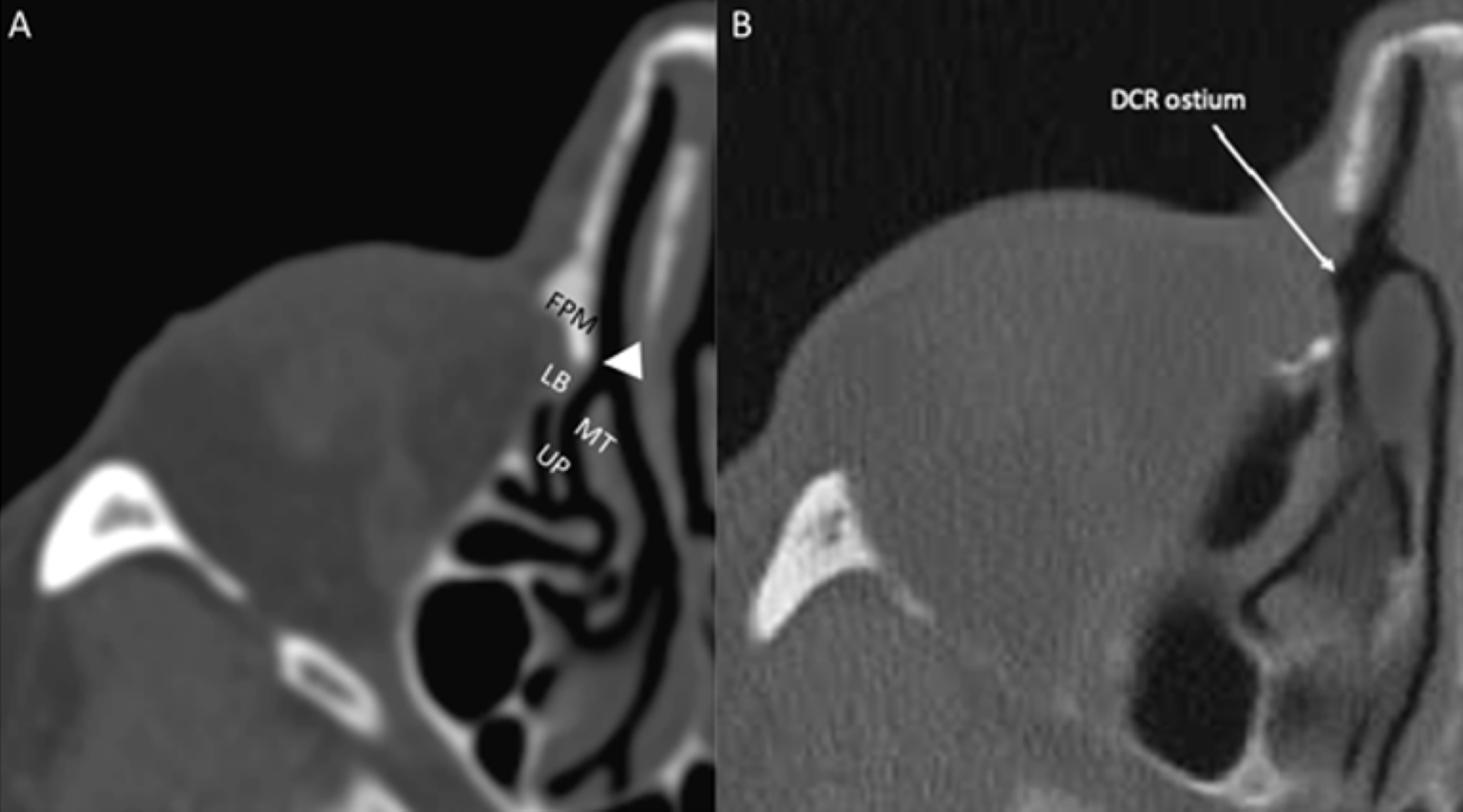
Figure 2 A-B
Figure 2A: Axial CT scan through the right orbit, bone window, focused on the lacrimal sac fossa and demonstrating the thicker bone of its anterior aspect formed by the frontal process of the maxilla (FPM) compared to the thinner posterior aspect formed by the lacrimal bone (LB), demarcated intranasally by the maxillary line (arrowhead). The uncinate process (UP) and middle turbinate (MT) are also seen.
Figure 2B: Axial CT scan through the right orbit, bone window, status-post endo-DCR, demonstrating wide osteotomy including removal of the anterior lacrimal sac fossa, affording a clear opening into the nasal cavity with clearance of the anterior aspect of the middle turbinate.
Chart Review
The team reviewed operative notes on 32 patients with primary acquired nasolacrimal duct obstruction who underwent one or more endo-DCR procedures aided by lacrimal sac transillumination. The 39 surgeries were conducted between April 2015 and October 2016.
Intraoperatively, the endoscopic point of transillumination was anterior to or involved the maxillary line in only seven cases (18%). In the other 32 cases (82%), it was entirely posterior to the maxillary line.
In all cases, the lacrimal sac was successfully accessed via osteotomy, beginning anterior to and including removal of the maxillary line. No major complications were observed.
Recommendations for Surgeons
When transitioning to endo-DCR, a light pipe can be a useful adjunct as long as the surgeon attends to anatomy:
- The key target for osteotomy creation is the intersection between the maxillary line and its confluence at the axilla of the middle turbinate
- Attend to the removal of the frontal process of the maxilla to incorporate proper anterior removal of bone
- As one progresses posteriorly, be aware of the root of the uncinate and do not disrupt the tissues within the middle meatus to avoid subsequent synechiae and possible sinus outflow obstruction
- While proceeding with the osteotomy superiorly, consider the possibility of an agger nasi cell
As an oculoplastic surgeon becomes more familiar with endo-DCR, a close working relationship with an otolaryngologist will be more helpful than using a light pipe. Ultimately, the oculoplastic surgeon will probably perform solo endo-DCR, but during the transition, great teaching can occur in both directions.
In addition, many patients who need endo-DCR benefit from adjunctive procedures, such as septoplasty and endoscopic sinus surgery, and it's important to identify these cases preoperatively through collaboration with an otolaryngologist.
view original journal article Subscription may be required
Learn more about the Department of Ophthalmology at Mass Eye and Ear/Mass General
Refer a patient to Mass Eye and Ear/Mass General