Redefining Cardiac Remodeling in the Athlete’s Heart
Key findings
- There is a need for a standardized and accurate framework to define associations between exercise and cardiac structure changes
- There is a strong relationship between training intensity and time, the resulting fitness and cardiac size (volume and mass)
- The current definition of cardiac remodeling has weaknesses
- The authors make the case for a combination of exercise intensity, duration and frequency as the major determinant of cardiac remodeling
Researchers are redefining the way we quantify cardiac remodeling in an athlete’s heart. Cardiac remodeling refers to the heart’s size, shape, structure and function and is currently measured by volume versus pressure load on the ventricle. In an August 2016 Cardiology Clinics article, researchers including Aaron L. Baggish, MD, associate director of the Cardiovascular Performance Program at Massachusetts General Hospital, argue that defining cardiac remodeling by volume versus pressure load is outdated. Instead, they introduce the concept of using two simple variables: exercise intensity and duration.
Subscribe to the latest updates from Cardiovascular Advances in Motion
Current Criteria for Cardiovascular Remodeling: Mitchell Criteria
The Mitchell Criteria were intended to assist with sports eligibility for patients with cardiovascular conditions such as cardiomyopathy. However, the criteria are often used as a schema for cardiac remodeling in research. They categorize sports by risks associated with explosive powers and measure the cardiovascular impact of exercise.
With this measure, a basketball player and a cross-country skier could be categorized together to anticipate cardiac remodeling--but these athletes are very different. Basketball players perform high-intensity exercise for minutes at a time over a set time period, while cross-country skiers maintain high-intensity exercise over a longer time period.
The Modern Definition of the Athlete’s Heart
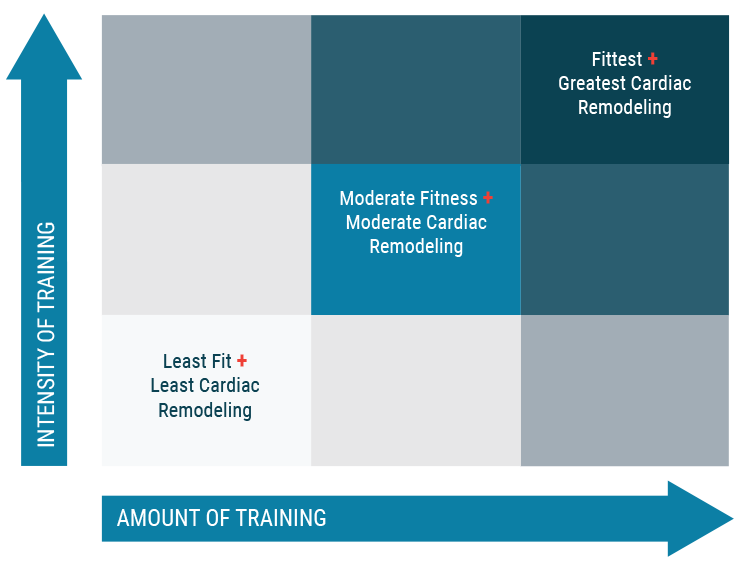
Fig. 1: A Simple Schema That Enables Anticipated Athletic Cardiac Remodeling from Measures of Exercise Intensity and Duration
The authors contend that the major determinant of cardiac remodeling is the amount of intensity multiplied by the duration and frequency of exercise, with a focus on the athlete rather than the sporting discipline. The new model recognizes the importance of evaluating the magnitude of the stress, which is determined by exercise intensity.
Greater amounts of training at high intensity promote fitness, which can be measured by VO2 max. The total amount of exercise performed at moderate or high intensity promotes an increase in VO2 max and cardiac remodeling. A strong correlation has been observed between cardiac size and VO2 max.
Using this new cardiac remodeling concept has some limitations because it does not incorporate the affects of age, race and gender. However, it has proven valuable for use in research studies and provides a simple model to use in the clinic.
Implications for Research
Ideally, athletic studies should attempt to accurately define the degree of athletic conditioning by exercise and duration. Connections between endurance exercise and some cardiac arrhythmias are increasingly prevalent, and the degree of exercise-induced cardiac remodeling is an underlying cause. Atrial fibrillation, for example, is more prevalent among endurance athletes. Researchers have linked atrial size to volumes of exercise and believe there may be a causal relationship. To study this relationship better, the authors argue that they can get a better estimate of cardiac remodeling using training time over intensity, which will better help define patient cohorts. VO2 max represents an essential standard for characterizing an athletic cohort.
Implications in the Clinic
Having the proper definition of cardiac remodeling is important in the clinic, for example, to differentiate between the athlete’s heart and an early dilated cardiomyopathy. Imaging techniques can aid in the assessment. An exercise test is also an important step to see whether the athlete’s fitness corresponds with cardiac enlargement.
This new cardiac remodeling schema can be used to advise patients with cardiac pathology on necessary exercise restrictions in a way that is easy to understand. The Mitchell Criteria guidance may be difficult to grasp. For example, a patient with hypertrophic cardiomyopathy may be told to only compete in 1A sports on the Mitchell Criteria. But what if the patient asks about riding her bike to work? In this instance, explaining exercise duration versus intensity could be useful in prescribing exercise in a logical and measurable way.
view original journal article Subscription may be required
Refer a Patient to the Cardiovascular Performance Program
Learn About the Corrigan Minehan Heart Center