Risk for Sudden Cardiac Death in Patients with SCAD
In This Article
- Incidence of spontaneous coronary artery dissection (SCAD) is rising due to increase in awareness and diagnostic advances, however optimal care for SCAD is unclear
- In this poster presented at Clinical Research Day at Mass General, data from a Mass General SCAD registry of 102 patients was reviewed
- There is a need for universal CPR training, awareness of risks of PCI in SCAD, and guidance about implantable cardioverter defibrillator (ICD) therapy given its use in current practice
- These preliminary results raise questions about whether ICD therapy risks outweigh the complications
Subscribe to the latest updates from Cardiovascular Advances in Motion
Introduction
Incidence of spontaneous coronary artery dissection (SCAD), defined as nontraumatic, non-iatrogenic and non-atherosclerotic separation of the coronary artery wall, is rising with the increase in awareness and diagnostic advances. Optimal management for SCAD is currently unclear. Data on cardiac arrest in SCAD is very scarce and there is no published literature on implantable cardioverter defibrillator (ICD) therapy in SCAD patients.
Methods
- Mass General SCAD Registry - patients who presented to Mass General with SCAD or were referred after a SCAD event:
- 102 patients
- 14 with cardiac arrest
- 7 with ICD placement
- Data gathered from chart review of SCAD hospitalization, patient survey and clinic visit with a Mass General cardiologist
Results
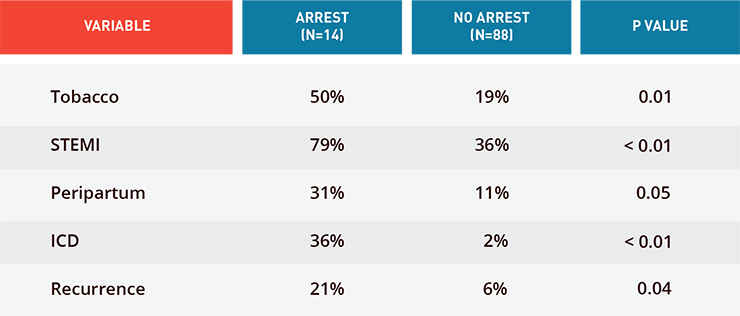
Fig. 1: Differences in Patients Presenting with SCAD with or Without Cardiac Arrest
- 7/14 cardiac arrests out-of-hospital, 4/14 in the emergency department and 3/14 during cardiac catheterization
- 5/7 ICDs placed for secondary prevention and 2/7 for primary prevention (inducible VT and recurrent NSVT)
- During mean follow up of 3.5 years, 1 ICD discharge for SVT and 1 patient with life-threatening ICD complications
- 4 patients received life vests in the setting of low ejection fraction. All had recovery of ejection fraction within 2 months resulting in discontinuation of life vest therapy
Conclusions
Cardiac Arrest in SCAD
- This was the largest cohort of SCAD patients with cardiac arrest ever assessed
- There is a need for universal CPR training, awareness of risks of PCI in SCAD, and guidance about ICD therapy given its use in current practice
ICD Therapy in SCAD
- ICD guidelines recommend therapy for 2° prevention in absence of reversible cause and for 1° prevention when low ejection fraction persists. It can be argued that SCAD patients meet neither criteria
- These preliminary results raise questions about whether ICD therapy risks outweigh the complications
- There is a need for a larger dataset through nationwide consolidation of SCAD registries
Shilpa Sharma MD1; Guy Rozen MD MHA2; Jessica Duran MD1; Theofanie Mela MD2; Malissa Wood MD2
1Medicine, MGH, Boston, MA, United States. 2Cardiology, MGH, Boston, MA, United States
Learn more about Mass General’s Coronary Intervention Program
Learn more about Mass General’s Spontaneous Coronary Artery Dissection Services